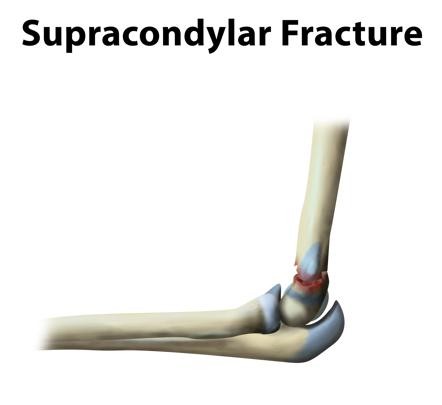
Supracondylar fractures constitute approximately 50% of all elbow fractures. The supracondylar region is thin and weak and thus it can fracture easily.
Fracture Types:
- Extension fracture
- Flexion fracture
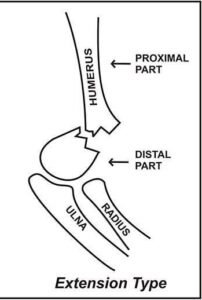
Extension type fracture:
- Most common type (95-98%)
- Occurs due to falling onto an outstretched hand.
- The distal fragment displaces posteriorly.
- Anterior interosseous neurapraxia (AIN) is the most common nerve palsy occurring with supracondylar fractures.
- Injury to the anterior interosseous nerve will lead to weakness of the flexor digitorum profundus muscle to the index finger and the flexor pollicis longus (FPL) muscle.
- The patient cannot do the OK sign or bend the tip of his index finger.
- Radial nerve neurapraxia is the second most common palsy and is evident by weakness in wrist and fingers extension.
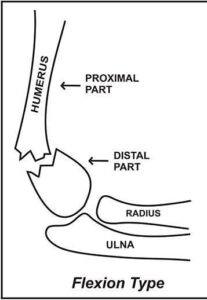
Flexion Type Fracture:
- It is rare and occurs due to falling directly on a flexed elbow.
- The distal fragment is displaced anteriorly.
- This type of fracture may be accompanied by Ulnar nerve neurapraxia.
- Injury of the Ulnar nerve will lead to loss of sensation along with the little finger.
- Later on, the patient may also have weakness of the intrinsic hand muscles and claws.
Garland’s Classification System:
Garland’s classification for supracondylar elbow fractures,
Type 1: This is a Non-displaced fracture.
Type 2: Is angulated with an intact posterior cortex
Type 3: This is a fracture showing complete displacement.
Type 4: Complete periosteal disruption and shows instability in both flexion and extension.

Radiology:
Plain Anterior-Posterior (AP) and lateral X-rays should be obtained.
A posterior fat pad sign seen on a lateral view X-ray should increase your suspicion of an occult fracture around the elbow.
Anterior humeral line:
- On a lateral view X-ray, the anterior humeral line is drawn along the anterior border of the distal humerus.
- Normally the anterior humeral line should run through the middle third of the capitellum.
- In extension type fractures the capitellum will be displaced posteriorly relative to the anterior humeral line.
Baumann’s Angle:
- Is formed by a line perpendicular to the axis of the humerus and a line going through the physis of the capitellum.
- Normally, Baumann’s angle should measure at least 11 degrees.
Examination:
- It is very important to assess the neurovascular structures.
- The Anterior interosseous nerve is assessed by asking the patient to do the OK sign with his hand.
- The Radial nerve is assessed by asking the patient to extend the wrist and fingers.
- The Ulnar nerve is initially assessed by loss of sensation along with the little finger. Later on, the patient may also have weakness of the intrinsic hand muscles and claws.
Treatment:
1. Non-operative treatment:
- Indicated for type 1 fractures.
- Usually consists of splinting or casting the elbow for a duration of 3-4 weeks.
- It is very important to remember not to flex the elbow in the splint or cast beyond 90 degrees in order to avoid vascular compromise and compartment syndrome.
2. Operative treatment:
- Type 2 and 3 fractures are usually treated by closed reduction and percutaneous pinning.
- During reduction, pronation of the forearm during elbow flexion helps to correct a Varus deformity.
- After reduction, check for a gap in the fracture.
- The neurovascular bundle may be trapped.
- Free the brachialis muscle from the fracture site, if it is inter-positioned.
- Fixation is usually achieved with 2-3 divergent lateral pins, depending on stability.
- Medial pins can also be added depending on stability.
- Open reduction is indicated only when closed techniques are unable to achieve the appropriate reduction of the fracture.
- Avoid posterior dissection to preserve vascularity of the fractures segment.
- Fracture reduction and fixation should be done emergently in cases of vascular compromise.
If you have any questions about Supracondylar Fracture please feel free and leave a comment.
Do share this blog with your friends and family!